Calcium Channel Blockers: How Metabolism Affects Drug Safety and Interactions
When you take a calcium channel blocker (CCB), you’re not just treating high blood pressure or chest pain-you’re introducing a drug that your body processes in a very specific, and sometimes dangerous, way. These medications are common: over 50 million Americans use them. But what most people don’t realize is that even a small change in how your body metabolizes them can lead to serious side effects-like fainting, dangerously low blood pressure, or even heart block. The real issue isn’t the drug itself. It’s what else you’re taking, what your liver can handle, and whether your body clears it the way it’s supposed to.
How Calcium Channel Blockers Work (and Why It Matters)
Calcium channel blockers stop calcium from entering heart and blood vessel cells. That relaxation of blood vessels lowers blood pressure. But not all CCBs are the same. There are two main types: dihydropyridines (DHPs) like amlodipine, nifedipine, and felodipine, and non-dihydropyridines (non-DHPs) like verapamil and diltiazem.
DHPs mainly affect blood vessels. That’s why they’re used for high blood pressure. Non-DHPs also slow down the heart’s electrical system. That’s why they’re used for arrhythmias or angina. But here’s the catch: their metabolic pathways are very different. And that difference changes everything when it comes to safety.
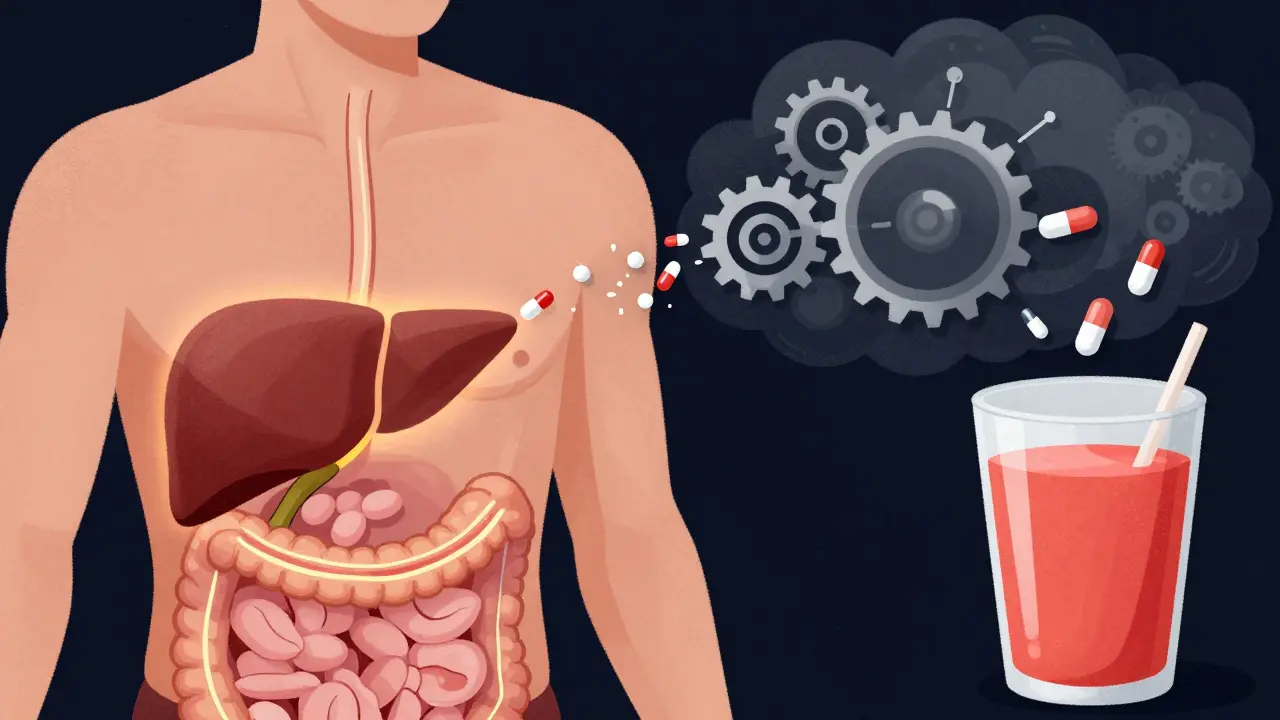
The Metabolic Engine: CYP3A4 and First-Pass Metabolism
Almost all calcium channel blockers are broken down by one enzyme: CYP3A4. This enzyme lives in your liver and gut. When you swallow a CCB, it gets absorbed and immediately hits this enzyme. About 80-90% of the drug is destroyed before it even enters your bloodstream. That’s called first-pass metabolism.
That’s why oral bioavailability is so low. Amlodipine? Only 64% makes it into your blood. Felodipine? Just 15%. That’s not a flaw-it’s how the system works. But when something blocks CYP3A4, the drug doesn’t get broken down. It builds up. And that’s where trouble starts.
Strong CYP3A4 inhibitors like ketoconazole, clarithromycin, ritonavir, and even grapefruit juice can reduce CCB clearance by 40% to over 70%. For someone taking verapamil, that could mean their blood levels jump from 100 ng/mL to 300 ng/mL overnight. That’s enough to cause severe bradycardia or low blood pressure. In some cases, it’s led to complete heart block-requiring a pacemaker.
Amlodipine vs. Verapamil: The Interaction Battle
Not all CCBs are created equal when it comes to interactions. Amlodipine is the quiet one. It’s metabolized by CYP3A4, but it doesn’t inhibit the enzyme. It’s also less affected by inhibitors because of its long half-life (30-50 hours). Even with grapefruit juice, most people don’t see dramatic spikes in blood levels.
Verapamil? Not so lucky. It’s not just a substrate of CYP3A4-it’s also a strong inhibitor. That means it can slow down the metabolism of other drugs. One study showed verapamil increases digoxin levels by 50-75%. That’s dangerous because digoxin has a narrow safety window. Too much, and you get nausea, confusion, or even fatal arrhythmias.
And then there’s diltiazem. It’s a moderate CYP3A4 inhibitor. Take it with simvastatin, and the statin’s blood levels can spike by 400%. That’s a recipe for rhabdomyolysis-a condition where muscle tissue breaks down and can damage your kidneys.
Here’s the bottom line: if you’re on multiple medications, amlodipine is the safest choice. Studies show only 12% of patients on amlodipine need a dose adjustment when on moderate CYP3A4 inhibitors. For diltiazem? That number jumps to 45%. Verapamil? It’s often contraindicated.
Who’s at Highest Risk?
You might think it’s just elderly people. And yes, they’re at higher risk-but not just because they’re older. It’s because they’re on more drugs. Over 58% of Medicare patients take five or more medications. Many of those drugs are CYP3A4 inhibitors.
Patients with liver problems? Their CYP3A4 activity drops. That means even normal doses can become toxic. Patients with kidney disease? Their metabolites don’t clear as well. And since 80-90% of CCBs leave the body through urine as metabolites, even a mild drop in kidney function (eGFR <60 mL/min) increases interaction risk by 47%.
And then there’s genetics. About 27% of people have genetic variants that make CYP3A4 work slower. These people are essentially born with a built-in interaction risk. Most doctors don’t test for this. But if you’ve had unexplained side effects from CCBs, it’s something to ask about.
Real-World Consequences
Patients aren’t just reading labels. They’re sharing experiences online. On Mayo Clinic’s patient forum, 68% of users who took CCBs with grapefruit juice reported dizziness or fainting. Nearly 50 needed emergency care. On Reddit’s r/Pharmacy, people described systolic blood pressure dropping 58 mmHg after combining diltiazem and verapamil. That’s not a typo-it’s a life-threatening drop.
One woman in her 70s was on amlodipine for hypertension. Her doctor added a new antibiotic for a sinus infection. Two days later, she collapsed at home. Her blood pressure was 72/40. She didn’t know grapefruit juice was a problem. Neither did her pharmacist. The antibiotic was a CYP3A4 inhibitor. Her amlodipine level tripled.
And it’s not just prescriptions. Over-the-counter supplements like St. John’s Wort, turmeric, and even some herbal teas can interfere. Many patients don’t tell their doctors about them. That’s how these interactions slip through.
What Doctors and Pharmacists Are Doing About It
Hospitals and clinics aren’t ignoring this. The Cleveland Clinic now requires CYP3A4 interaction screening for every new CCB prescription. That’s not optional. It’s protocol. And it’s working. They found 23% of patients were at high risk before even starting the drug.
For those patients, they start with amlodipine at 2.5 mg-not the usual 5 mg. That small change reduces risk by 60%. And it’s being adopted: 78% of clinics now follow this guideline.
Community pharmacists are spending an average of 12.7 minutes per CCB prescription checking for interactions. That’s more than double the time they spend on other blood pressure meds. And they’re catching 18% of dangerous combinations before the patient leaves the pharmacy.
Electronic health records now have mandatory alerts. If you’re on verapamil and your doctor tries to prescribe clarithromycin, the system pops up: “High risk of heart block. Avoid combination.” Epic Systems saw a 42% drop in severe interactions after adding these alerts in 2022.
What You Should Do Right Now
If you’re on a calcium channel blocker, here’s what you need to do:
- Make a full list of everything you take-prescriptions, OTC meds, supplements, even herbal teas.
- Check if any of them are CYP3A4 inhibitors. Common ones: grapefruit juice, ketoconazole, clarithromycin, ritonavir, diltiazem, verapamil, fluconazole, and St. John’s Wort.
- If you’re on verapamil or diltiazem, ask your doctor if amlodipine might be safer.
- If you’re over 65 or have kidney/liver issues, ask about dose adjustments. Amlodipine often doesn’t need them. Verapamil usually does.
- Never start a new medication without asking: “Could this interact with my blood pressure pill?”
And if you’re taking amlodipine? You’re probably fine. But don’t assume. Even amlodipine can become risky if you’re on multiple inhibitors or have poor liver function.
The Future: Personalized Dosing and Genetic Testing
The FDA approved a tool called CCB-Check in 2023. It integrates with hospital systems and gives real-time risk scores. In its first six months, it cut hospitalizations from CCB interactions by 31%.
And research is moving faster. Scientists are now studying how gut bacteria affect CCB metabolism. One study found 34% of clearance differences could be traced to microbiome differences. That means two people on the same dose, with the same liver function, could have completely different outcomes.
By 2027, personalized dosing based on genetics, liver function, and even gut health may become standard. But for now, the safest approach is simple: know your drugs, know your risks, and don’t assume your doctor knows everything you’re taking.
Can grapefruit juice really affect calcium channel blockers?
Yes. Grapefruit juice is one of the strongest natural CYP3A4 inhibitors. It can increase blood levels of amlodipine by 40%, verapamil by 60%, and diltiazem by over 70%. In one study, 68% of patients taking CCBs with grapefruit juice reported dizziness or fainting. Even one glass a day can be dangerous. Avoid it completely if you’re on any CCB.
Why is amlodipine considered safer than other calcium channel blockers?
Amlodipine has a long half-life (30-50 hours), which means it builds up slowly and doesn’t spike dangerously. It’s also not an inhibitor of CYP3A4, so it doesn’t interfere with other drugs. Studies show only 12% of patients on amlodipine need dose changes when on other CYP3A4 inhibitors, compared to 45% for diltiazem and often complete avoidance for verapamil. It’s the most interaction-friendly CCB available.
Do I need blood tests if I’m on a calcium channel blocker?
Routine blood tests aren’t required for most people. But if you’re on verapamil or diltiazem and also taking other medications like statins, antibiotics, or antifungals, your doctor may recommend therapeutic drug monitoring. For verapamil, the safe range is 50-150 ng/mL. Levels above 200 ng/mL can cause heart block. Only 32% of community clinics do this testing, so ask if you’re at risk.
Can kidney disease affect how calcium channel blockers work?
Yes. While less than 1% of CCBs are excreted unchanged in urine, 80-90% leave the body as metabolites. If your kidneys are weak (eGFR below 60 mL/min), those metabolites build up. This doesn’t affect amlodipine much, but verapamil requires a 50% dose reduction in moderate kidney disease. Diltiazem may also need adjustment. Always tell your doctor if you have kidney issues.
What should I do if I start a new medication while on a calcium channel blocker?
Stop and check. Don’t assume it’s safe. Ask your pharmacist: “Is this safe with my blood pressure pill?” Many new medications-antibiotics, antifungals, even some antidepressants-are CYP3A4 inhibitors. If you’re on verapamil or diltiazem, the risk is higher. If you’re on amlodipine, the risk is lower but still real. Always get a second opinion before combining drugs.
Next Steps: What to Do If You’re at Risk
If you’re over 65, on multiple medications, or have liver or kidney problems, don’t wait for a side effect to happen. Schedule a medication review with your pharmacist or doctor. Bring all your bottles-even the ones you take “only when needed.”
Ask specifically: “Am I on a CCB? Is it amlodipine? Could any of my other meds be interacting with it?” If you’re on verapamil or diltiazem, ask if switching to amlodipine is an option.
And if you’ve ever felt dizzy, lightheaded, or had your heart skip after starting a new drug, tell your doctor. That could be a CCB interaction. It’s not just “getting older.” It’s a metabolic problem-and it’s fixable.
I've been on amlodipine for five years now. My BP was 170/105 before. Now it's 118/72. No dizziness, no fatigue, no weird side effects. But last month my doc put me on a new antibiotic for a sinus infection - clarithromycin. I felt like I was going to pass out walking to the fridge. Took me three days to realize it was the combo. My pharmacist should've warned me. They don't. They just hand you the script and say 'take as directed.' Like that's enough. This isn't just about drugs - it's about how broken our system is.
i read this and thought 'oh god not another medical post' but then i saw grapefruit juice and i was hooked. i eat half a grapefruit every morning. like, it's healthy right? turns out i'm basically poisoning myself with my breakfast. my mom took verapamil and ended up in the er after drinking grapefruit juice for a week. she thought it was 'just juice.' now she drinks orange juice and cries about it. i feel bad for her. but also... why didn't anyone tell us?
This is why I don't trust Big Pharma. They know exactly how dangerous these interactions are. They market these drugs like they're candy. And then when someone ends up in the hospital? They blame the patient. 'You didn't read the label.' But the label is printed in 6-point font on a tiny slip of paper. And if you're over 65? You probably can't read it anyway. This isn't an accident. It's negligence. They profit off your confusion. I'm not taking another pill until I get a full metabolic panel and a lawyer.
I’ve been wondering why my grandma keeps fainting… turns out she’s on simvastatin + diltiazem + grapefruit juice. She swears the juice helps her digestion. I tried to tell her. She said 'you’re just scared of big pharma.' Now I’m scared of her. I think someone’s poisoning her. Maybe the pharmacy? Maybe the government? I looked up CYP3A4 on Wikipedia and now I think my water is being altered. I need a Geiger counter for my vitamins.
The tragedy of modern pharmacology is not that drugs are dangerous - it is that we have elevated convenience above comprehension. We swallow pills like they are chocolates at a funeral. We do not pause. We do not question. We do not honor the sacred complexity of the human liver. And when the body rebels - when the heart stutters, when the blood pressure plummets - we blame the patient. We do not ask: who taught us to trust a pill? Who sold us the illusion of safety? The answer is not in the lab. It is in the boardroom.
Amlodipine is the safest. End of story.
Just wanted to add - if you're on any of these meds and you're also taking St. John’s Wort, turmeric supplements, or even some herbal teas like green tea in large amounts, those can also interfere with CYP3A4. Not as strongly as grapefruit or antibiotics, but cumulatively? It adds up. I’m a nurse and I’ve seen three cases in the last year where patients didn’t realize their 'natural' supplements were the problem. Always talk to your pharmacist. They’re the unsung heroes.
I live in India and we have so many people on blood pressure meds here. But no one talks about interactions. My uncle was on diltiazem and took a cheap antibiotic from the local shop - turned out it was a CYP3A4 inhibitor. He ended up in a coma for 3 days. We didn’t even know what CYP3A4 meant. Now I print out these charts and stick them on the fridge. Knowledge is power - but only if someone tells you.
This is SO important!! I’m a med student and I just had a patient on verapamil who started taking ketoconazole for a fungal infection - she went into complete heart block. We had to shock her twice. She’s fine now, but she had no idea. I showed her the chart on CYP3A4 interactions and she cried. I wish every patient got this info before they left the pharmacy. We need warning stickers. Like on cigarette packs. PLEASE. Someone make this a public health campaign!!
so u mean to tell me that my morning grapefruit smoothie is secretly a heart attack waiting to happen? wow. thanks for the info, doctor. next u gonna tell me breathing is dangerous. i mean, i get it. but can we please stop acting like every human is a walking pharmacology exam? i took amlodipine for 8 years. never had an issue. maybe the real problem is overmedicating people who don’t need it.
The data presented is accurate and aligns with current clinical guidelines. However, the framing of risk as absolute rather than probabilistic may lead to unnecessary patient anxiety. CYP3A4 inhibition varies widely between individuals due to genetic polymorphisms, age, and concurrent disease states. A population-level warning without individualized risk stratification may do more harm than good. I recommend clinicians use tools like the Liverpool CYP3A4 Interaction Checker before making changes.
You people act like drugs are magic. They’re just chemicals. Your liver doesn’t care about your birthday. It doesn’t love you. It just breaks things down. If you can’t handle that? Stop taking pills. Or better yet - stop pretending your body is a temple. It’s a factory. And factories break. That’s why they have maintenance schedules. You? You’re just lazy.